
Why the newborn reaches the outside world in a supposedly Vitamin K deficient state requiring immediate supplementation with an essential vitamin has not yet been explained. Is it really a flaw in our design or could it actually confer us intelligent biological advantages?
The phenomena of low newborn vitamin K levels are not isolated to humans but extend to all mammals and bird life as well. This should be a massive clue for us all that we are indeed interfering with natural purposeful physiology.
The three prevailing theories for newborn Vitamin K deficiency are –
1. The less viscous and sticky our blood eg, lower levels of coagulant factors the more unhindered fetal stem cells can traverse the circulatory system to sites of trauma that may have occurred during birth. All babies regardless of how gentle or hands off the birth likely sustain micro traumas on their travel through the pelvis. Sticky, thick sludgy blood that is 20 x more viscous than an adults means less movement of stem cells to sites of tissue injury. This is of course still dependent upon delayed cord clamping occurring – wait till white.
2. Maintaining Vitamin K in the infant at a cellular concentrations only just sufficient ( what we call ‘deficient’) to meet the immediate metabolic needs is not an accident and may reduce the risk of mutagenic events during a period of rapid cell proliferation. Creating a situation of cellular excess of K by way of administering an adult dose of synthetic K at birth could be creating carcinogenic or mutagenic metabolites which the infant doesn’t yet have the capacity to excrete. (Pediatr Res 22: 405-408, 1987).
3. In order to absorb vitamin K we have to have a functioning biliary and pancreas system. An infant’s digestive system isn’t fully developed at birth. Too much vitamin K could tax the liver. As baby ages and the digestive tract, mucosal lining, gut flora, and enzyme functions develop and mature, baby can process more vitamin K.
This got me thinking about the earlier version of the K shot offered Konakion MM Paediatric K by Roche which was introduced in the 1950’s. Konakion was a cremophor formulation for IM injection which contained the adjuvants propylene glycol, phenol and polyethylated castor oil.
In 1992 an association between Intramuscular use of the cremophor Vitamin K formulation and childhood cancer arose. Subsequent studies confirmed a ‘consistent small but non-significant trend towards an increased incidence of acute lymphoblastic leukaemia’ in children who received it (reviewed by Von Kries 1998, Wariyar et al 2000).
The cremophor formulation was ceased in 2000 and the adjuvants were replaced with Glycocholic acid, Lecithin (322), Sodium hydroxide, Hydrochloric acid (507) for a supposedly safer concoction.
So was it the adjuvants in the earlier version of Konakion responsible for increased cancer risk or simply the huge amount of K delivered in the dose that created toxigenic and carcinogenic cell mutations leading to childhood leukemia?
Science has concluded that low levels of vitamin K in the cord plasma of the normal newborn are perfectly normal physiology however, are still significantly impacted by maternal Vitamin K deposits and pregnancy deficiency.
Women are enthusiastically advised (coerced and blackmailed) into believing that Vitamin K in Konakion form antenatally is the best method of preventing possible ‘vitamin K deficiency bleeding’ in infants thanks to Big Pharma’s peddling when available research clearly demonstrates that actually, if mum just made sure she was getting abundant Vitamin K1&2 in her diet, she and her baby would be just as well protected……naturally.
“Particularly in preterm pregnancies, little vitamin K actually crosses the placenta from mother to infant [94]. However, this could be attributed to insufficient maternal levels of vitamin K in the first place. In fact, several studies have demonstrated that supplementation with vitamin K in more advanced pregnancy increases plasma concentrations of this nutrient and enhances coagulation function of future mothers [92]. In addition, administration of vitamin K supplement to pregnant women resulted in improved vitamin K-dependent coagulation factors in umbilical blood and reduced the incidence as well as the severity degree of periventricular-intraventricular hemorrhage (PIVH) in premature infants [95,96]. Furthermore, late-preterm babies, whose mothers were given vitamin K supplementation at imminent risk of preterm labor, were able to achieve a clotting status approaching that of full-term neonates and are less liable to develop PIVH [97]…….This argument should encourage breast-feeding mothers to seriously consider supplementation with vitamin K2.” – International Children’s Health Journal.
Reasons why Vitamin K may be low at birth include –
1. Poor placental transfer of vitamin K due to low maternal deposits.
2. Breast milk is low in vitamin K due to low maternal availability.
3. Newborn gut flora is immature and cannot yet synthesize its own Vitamin K2, this may also contribute to vitamin K malabsorption in early infancy.
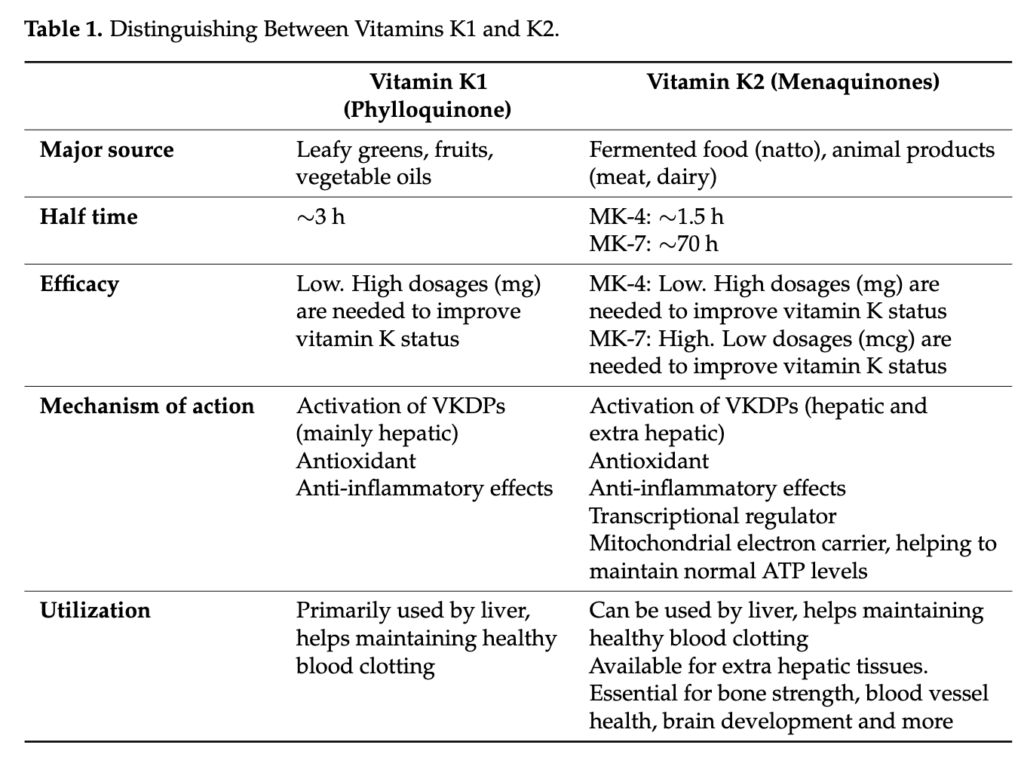
Phylloquinone (K1) and menaquinones (MK-4, MK-6, and MK-7) are routinely found in placentas and maternal plasma. K1 and MK-4 were found in umbilical cord plasma. The evidence is clear that the various forms of Vitamin K can indeed be taken up by the fetus in utero thus highlighting that dietary intake of Vitamin K most definitely can make a difference. Prophylactic maternal supplementation coupled with dietary intake should be the focus for infant well-being over the dangerously high dose of synthetic, adjuvant spiked pharmaceutical Konakion.
The amount of vitamin K in breast milk can be increased by maternal intake of supplemental vitamin K (Greer 1999) and can confer a newborn infant with enough clotting factors to prevent risk of VKDS or PIVH. Straight from a statement by the Paediatric Division of the Royal Australasian College of Physicians yet it’s not encouraged…. why? Big Pharma is why.
Japan and the Netherlands have the highest Vitamin K breast milk concentrations owing to their abundant consumption of natto and raw grass fed cheeses.

The standard western diet scrapes the bottom of the barrel when it comes to K2 intake of all forms and research indicates that even where excellent diet prevails we are still falling short of optimal K2 supply which is where supplementation can be so helpful.
The stupidity of a system that advises the Western pregnant woman to avoid alllll the Vitamin K2 abundant foods eg, duck, goose and chicken liver, raw cheese such as Gouda, too many egg yolks etc cannot be ignored. Nettle Tea and dark leafy greens afford us excellent K1 sources which the body can in turn synthesis into K2.
Supplement wise, Innovix K2 and Emu Oil are my two top full spectrum K2 supplements. The current adequate intake level of vitamin K for pregnant and nursing women is suggested as 90 mcg a day. However this really is likely a third of what our body truly needs to thrive. Likewise, research suggests that 45–50 mcg/day MK4-7 is an appropriate intake range for children but 100mcg is a more realistic recommendation.
Although the practice of prophylactic Vitamin K is now almost routine in North America and Australia, the basis of this regimen is still questioned elsewhere. The controversy arises from the fact that we are intervening in a natural phenomenon. Why the normal newborn reaches the outside world in a state requiring immediate supplementation with an essential vitamin has not been explained and yet we are arrogant enough to believe it must be a defect that requires ‘fixing’ with an ill conceived pharmaceutical drug.
As always, love hearing your thoughts, opinions and experiences.



0 Comments